设为首页
收藏本站
开启辅助访问
切换到窄版
患者服务:
与癌共舞小助手
微信号:
yagw_help22
您好!请先
登录
或
注册
登录后查看更多精彩内容...
只需一步,快速开始
手机号快速注册登录
快捷导航
搜索
首页
Portal
社区
BBS
临床入组
直播
微信精华
APP
健康资讯
搜索
热搜:
2992
用药讨论
肺腺癌十年
特罗凯
184
凯美纳
阿西替尼
胃癌
胸痛
多吉美
索坦
4002
脑转
二线化疗
DCA
腹胀
恶心
发烧
淋巴
腋下
气喘
装药
与癌共舞
»
社区
›
交流分区
›
非小细胞肺专区
›
罕见突变——MET专区
›
MET Y1230H 有关的猜想 (不构成任何建议) ...
[咨询交流]
MET Y1230H 有关的猜想 (不构成任何建议)
[复制链接]
微信扫一扫 分享朋友圈
已有
33695
人穿越成功
教程:手机怎么扫描二维码
1671924
330
吕超
发表于 2022-3-14 12:54:16
|
置顶
|
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-7-3 21:08:11
来自手机
|
显示全部楼层
来自: 中国
大家千万注意丹毒
登录/注册后可看大图
来自苹果APP客户端
举报
使用道具
回复
支持
1
反对
0
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-28 11:04:59
来自手机
|
显示全部楼层
来自: 中国
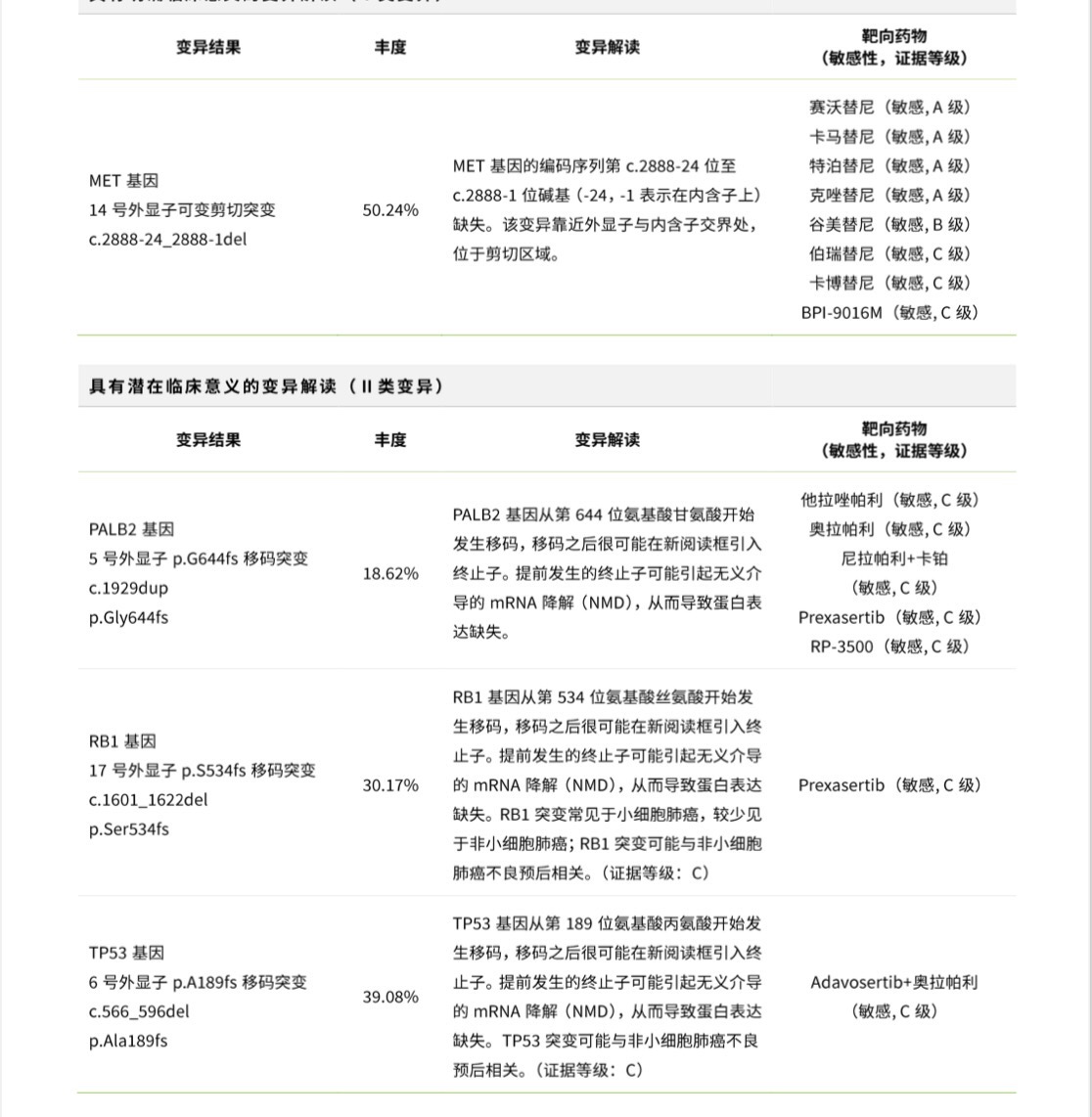
MET 耐药也有这种方式,RB1 TP53组合
登录/注册后可看大图
来自苹果APP客户端
举报
使用道具
回复
支持
1
反对
0
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-27 21:02:55
来自手机
|
显示全部楼层
来自: 中国
这句话需要仔细分析一下,会不会毒性增加很大。
登录/注册后可看大图
来自苹果APP客户端
举报
使用道具
回复
支持
1
反对
0
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-25 22:20:13
来自手机
|
显示全部楼层
来自: 中国
登录/注册后可看大图
来自苹果APP客户端
举报
使用道具
回复
支持
1
反对
0
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-22 09:07:36
来自手机
|
显示全部楼层
来自: 中国
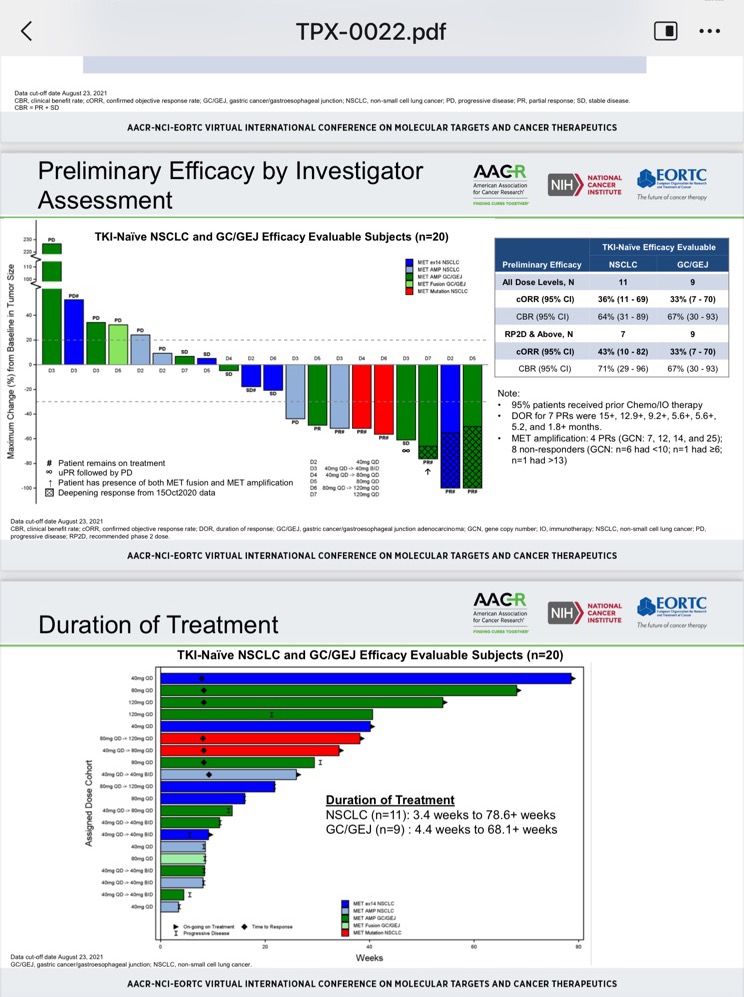
TPX-0022 还是值得期待的
登录/注册后可看大图
来自安卓APP客户端
举报
使用道具
回复
支持
1
反对
0
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-22 08:59:02
来自手机
|
显示全部楼层
来自: 中国
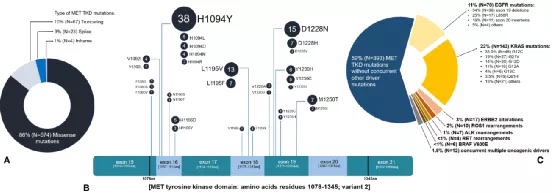
MET酪氨酸激酶结构域(MET TKD)突变
在人口统计学数据可用的患者中,与MET14号外显子跳跃突变NSCLC患者(N=390)相比,MET TKD突变NSCLC患者(N=75)明显更年轻(中位年龄63岁vs 73岁,p<0.0001),不过性别和自我报告的种族无显著差异。
668个MET TKD突变中,525个突变的致病意义不明确,143个(21.4%)具有已知的致癌潜力,包括MET H1094Y/L/D/N/R、D1228N/H/V、L1995V/F、M1250T/I、Y1230H/C/G
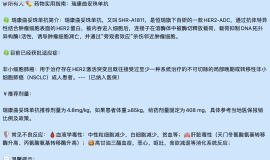
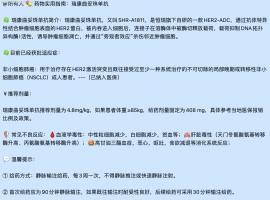
病例分享:研究人员还分享了2例MET TKD突变(未检测到其他驱动基因突变)NSCLC患者采用MET-TKI[Elzovantinib(TPX-0022)]治疗的疗效。其中1例为携带MET H1094Y突变的64岁男性肺腺癌患者,经Elzovantinib治疗后,肿瘤缩小-56.8%,达到部分缓解(图3A);另一例为携带MET F1200I突变的80岁男性NSCLC患者,治疗后肿瘤缩小-51.4%,亦达到部分缓解
登录/注册后可看大图
来自安卓APP客户端
举报
使用道具
回复
支持
反对
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-20 10:41:11
来自手机
|
显示全部楼层
来自: 中国
抗生素与免疫 有分歧
登录/注册后可看大图
来自苹果APP客户端
举报
使用道具
回复
支持
反对
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-17 23:47:12
来自手机
|
显示全部楼层
来自: 中国
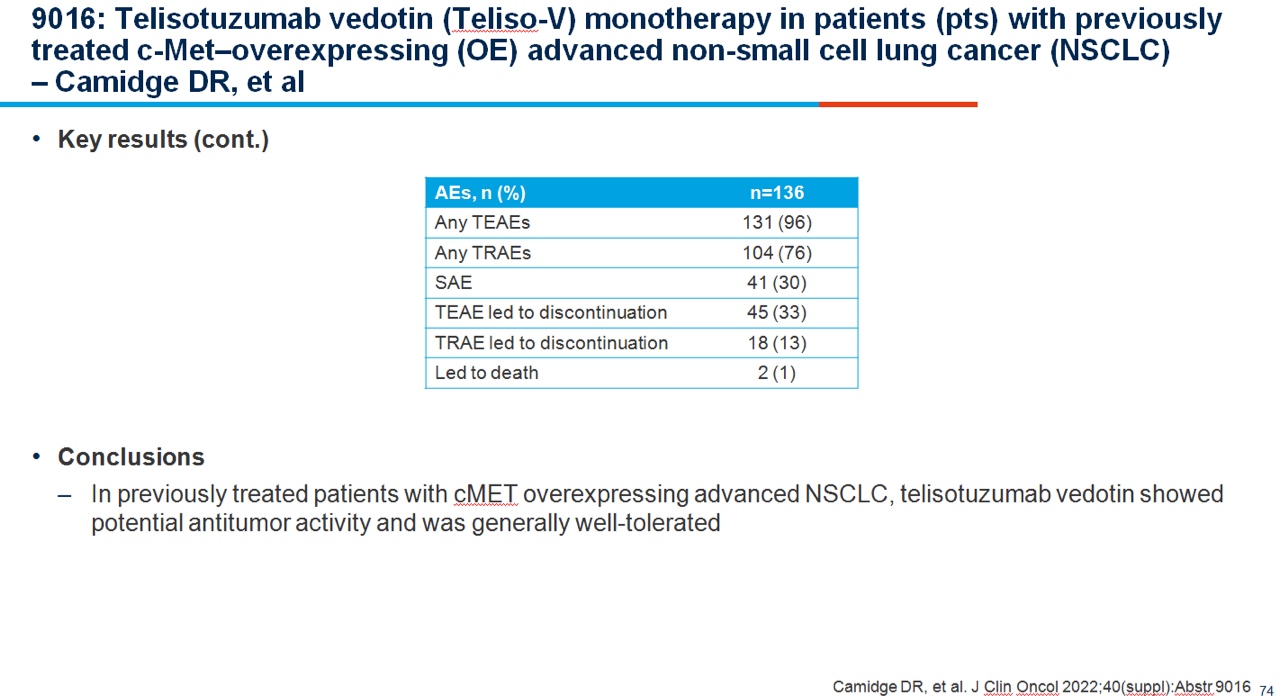
副作用巨大
登录/注册后可看大图
登录/注册后可看大图
来自苹果APP客户端
举报
使用道具
回复
支持
反对
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-16 14:43:47
来自手机
|
显示全部楼层
来自: 中国
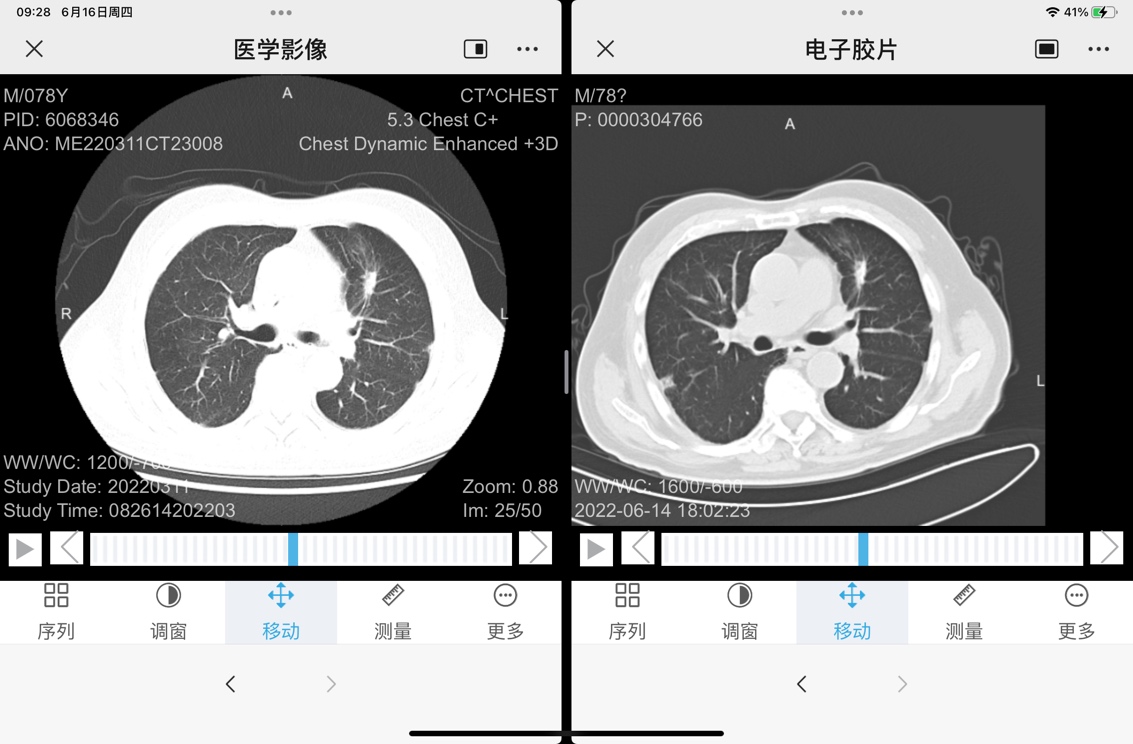
左肺上叶蛇端部分钙化,右肺靠近右侧有个新发奇怪的结节,外面强化,里面弱不符合恶性肿瘤的特点,报告也没提。
登录/注册后可看大图
来自安卓APP客户端
举报
使用道具
回复
支持
反对
显身卡
尚未签到
个人资料
主题列表
发消息
吕超
大学三年级
发表于 2022-6-16 06:36:15
来自手机
|
显示全部楼层
来自: 中国
在搜索引擎中输入关键词“科利毒素“,你会惊讶地发现,在一个世纪前,癌症免疫治疗先驱威廉·科利(William Coley,1862-1936)医生通过人为制造丹毒感染,成功治愈了众多癌症患者,但因为治疗效果不稳定(存在因感染而死亡的病例),医学界权威没有认可他的方法。
新冠肆虐以来,人们惊奇地发现,一位恶性淋巴瘤患者感染新冠病毒后,体内的肿瘤在未给予激素治疗、化疗、免疫治疗的情况下大面积消失。
在近年来国外的一些研究中发现,高乳酸环境既促进了癌细胞的生长与增殖,甚至是癌细胞存活的条件,也促进了癌细胞的转移。但是,细菌和病毒感染都会导致血乳酸水平的升高,表面上看,这与上述现象明显是矛盾的。如何解释呢?
以下是我的分析,纯属个人观点。
首先,一个基本的事实是,感染会导致毛细血管壁通透性的增加,这已为大量的研究所证实。
当毛细血管壁的通透性正常时,当细胞间液中的乳酸含量正常时,血液中的乳酸含量也处在正常水平。当细胞分泌大量乳酸时,血液中的乳酸含量也随之升高。
但是,如果毛细血管壁的通透性下降,即使细胞间液中的乳酸含量高于正常值(癌细胞周围的细胞间液就是这样),血液中的乳酸含量并不会等比例升高,其升高幅度低于细胞间液中的乳酸含量升高的幅度。当毛细血管壁通透性增加时,甚至超过正常水平时,细胞间液与血液中的乳酸浓度才会趋于一致。
另一个研究发现是,所有的癌症患者都存在着微循环障碍。
如果,癌细胞的增殖与转移依赖于高于正常值的乳酸浓度这一结论是正确的,那么:
尽管感染使细胞分泌了更多的乳酸,由于毛细血管壁通透性的急剧增加,导致乳酸大量进入血液并被带离,反而存在癌细胞间液的乳酸水平降低的可能,进而抑制了癌细胞的分裂,甚至导致癌细胞死亡,出现癌症自愈现象。
以上都是非定量的分析与猜测,仅供参考。
来自苹果APP客户端
举报
使用道具
回复
支持
反对
显身卡
查看下一页
返回列表
1 ...
7
8
9
10
11
12
13
14
15
... 33
/ 33 页
下一页
发表回复
高级模式
B
Color
Image
Link
Quote
Code
Smilies
您需要登录后才可以回帖
登录
|
立即注册
本版积分规则
发表回复
回帖并转播
回帖后跳转到最后一页
发表新主题
回复
转播
评分
分享
版块推荐
百宝箱
前沿信息
临床入组
初识癌症
就医信息
微信精华
跨越五年
综合交流
肺部分区
肝部分区
胆管分区
肾部分区
肠部分区
妇科分区
EGFR(HER2)
查看论坛所有版块>>
每日签到
我的收藏
我的帖子
我的好友
个人设置
我的消息
我的提醒
我的听众
我的点评
管理工作
坛友互动
门户管理
管理中心
退出登录
与癌共舞
天猫旗舰店
签到
连续天
8人
签到看排名
更多>
精彩推荐
汇总4月最新:临床试验招募| 小细胞肺
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。 ...
重生第120天
明天继续第五疗,继续升级打怪 ...
脑膜转移诊疗潘振宇教授科普总结
脑膜转移诊疗潘振宇教授科普总结 脑膜转移 中位治疗生存期 3-6月 脑膜转移的临床 ...
更多>
热点动态
1.
汇总4月最新:临床试验招募| 小细胞肺癌
2.
太难了
3.
老挝9291
4.
2026年4月13日签到记录贴
5.
肺腺癌伏美耐药求助
6.
芦康 我的小理解
7.
谁家有卡马替尼
8.
重生第120天
更多>
随手拍
汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。 临
重生第120天
明天继续第五疗,继续升级打怪
脑膜转移诊疗潘振宇教授科普总结
脑膜转移诊疗潘振宇教授科普总结 脑膜转移 中位治疗生存期 3-6月 脑膜转移的临床表现
新人求助
我爸爸身体不适 26 年 4 月 10 号去医院检查,初步结果是肺肿可能是肺癌,因年纪大 7
咨询大家一下
咨询大家一下,我们22年1月份查出来肺腺癌四期,化疗6次,信迪利单抗联合到第9次培美
帮助中心
网友中心
购买须知
支付方式
服务支持
资源下载
售后服务
定制流程
关于我们
关于我们
友情链接
联系我们
关注我们
官方微博
官方空间
微信公号
022-68288305
邮箱:kefu@yuaigongwu.com
工作时间9:30-17:30
Copyright © 2008-2024
与癌共舞
https://www.yuaigongwu.com/ 版权所有 All Rights Reserved.
Powered by
Discuz!
X3.5 技术支持:
克米设计
(
京ICP备12008483号-1
|
11011102001537
)
快速回复
返回顶部
返回列表






 显身卡
显身卡